Retinal Laser Treatment
Retinal laser is a valuable tool in the treatment of diabetic eye disease and retinal vein occlusion, and in the treatment of retinal tears in patients presenting with flashes and floaters.
Three forms of laser are used:
- Panretinal photocoagulation (PRP) suppresses abnormal new blood vessels in diabetic retinopathy and retinal vein occlusion.
- Focal or grid laser — a gentler form — helps manage macular oedema.
- Laser retinopexy seals retinal tears and reduces the risk of retinal detachment.
All three are performed in the consulting room using a slit lamp.
Panretinal Photocoagulation (PRP) for Diabetic Retinopathy and Retinal Vein Occlusion
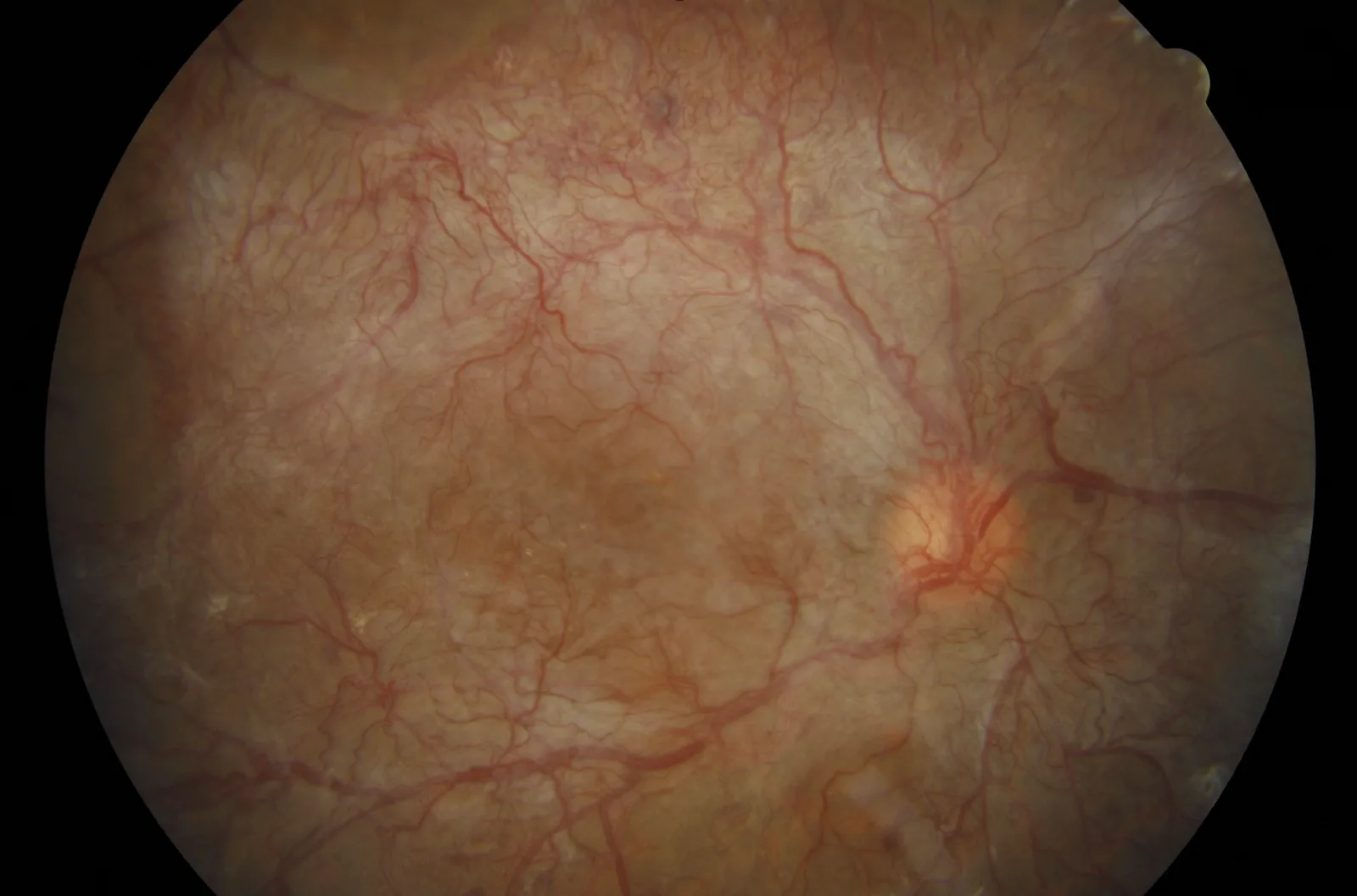
In proliferative diabetic retinopathy and severe retinal vein occlusion, areas of the retina become starved of oxygen and release chemical signals (VEGF) that drive the growth of fragile, abnormal new blood vessels. These vessels can bleed into the eye, pull on the retina, or trigger neovascular glaucoma. PRP treats the affected peripheral retina to remove that signal, helping to protect central vision and reduce the risk of these complications.
Why regular review matters
If neovascularisation is present, PRP is needed — but it rarely causes symptoms, and is almost always detected at a routine retinal review before the patient is aware anything is wrong. Patients who are never screened can present very late: either with sudden vision loss from bleeding into the eye, or with scar tissue from the abnormal vessels pulling the retina out of position.
The patient in the image above was one of these late presentations. Treatment was extremely difficult — surgery combined with laser and injections — and the outcome was only moderate. Regular retinal review is the difference between catching neovascularisation early and treating it late, and for patients with diabetes it is one of the strongest reasons to keep up with monitoring even when vision feels normal.
Focal or Grid Laser for Macular Oedema
Before the introduction of intravitreal injections, focal or grid laser was the main treatment for macular oedema. Anti-VEGF injections have largely replaced it as first-line therapy because they tend to give better visual outcomes for centre-involving disease — but focal laser remains a useful option in selected patients, particularly where leakage is away from the central macula.
Laser Retinopexy for Retinal Tears
Retinal tears are an entirely different problem from the conditions above. They are not a complication of diabetes or retinal vein occlusion — they arise from age-related changes in the vitreous gel inside the eye (posterior vitreous detachment), and patients almost always present with new flashes and floaters rather than as part of ongoing retinal care.
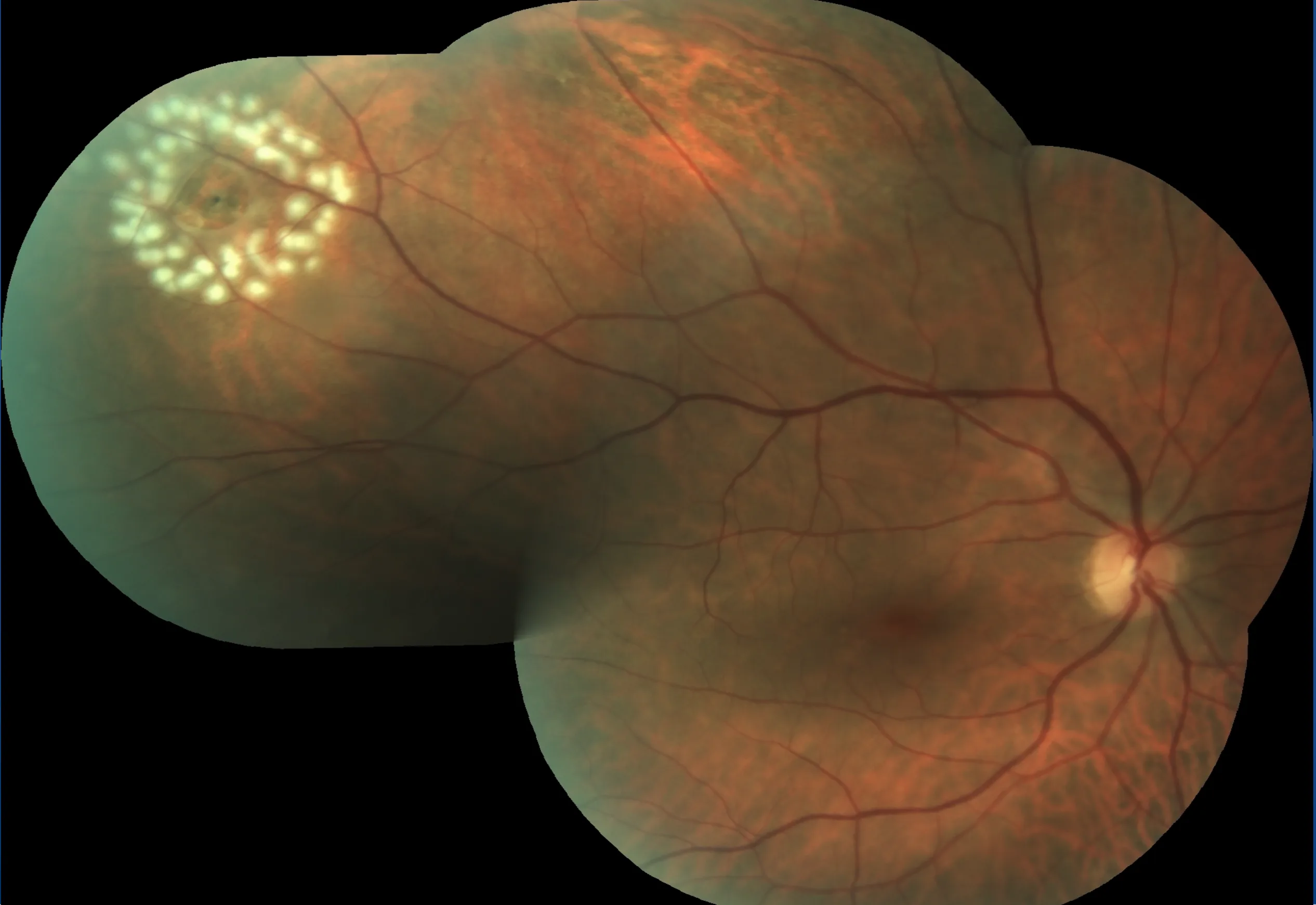
When a small tear develops in the retina, fluid can pass underneath and lift the retina away — a retinal detachment. Laser retinopexy creates a barrier of small burns around the tear, forming a scar that bonds the retina to the underlying tissue and limits fluid from spreading. It is generally effective when performed early, before any detachment has developed.
When It Is Urgent
New flashes, a sudden increase in floaters, or a shadow or curtain in vision should be assessed urgently. These may indicate a retinal tear or early detachment.
The Procedure
Both PRP and laser retinopexy are performed in the consulting room using a slit lamp.

- Anaesthetic drops are applied
- A contact lens is placed on the eye to focus the treatment
- Laser spots are applied to the retina in a controlled pattern
Retinopexy is usually completed in a single session of a few minutes. PRP takes longer and may be staged over more than one visit, particularly when the area requiring treatment is large.
What Does It Feel Like?
Patients may notice brief flashes of light, mild discomfort, stinging, or aching during treatment. The sensation varies with the intensity and extent of laser required — focal retinopexy is generally well tolerated, while extensive PRP can be more uncomfortable and is often staged for that reason.
After the Procedure
Vision may be slightly blurred temporarily, with some glare, light sensitivity, or transient ache. Following extensive PRP, there may be some reduction in peripheral or night vision — this reflects the trade-off of the treatment, sacrificing some peripheral function to protect central vision.
After laser retinopexy, the seal takes time to form fully, and activity restrictions may be advised in the early period. Follow-up confirms whether the treatment has been effective and whether further treatment is needed.
Risks
- Temporary blur or light sensitivity
- Reduced peripheral or night vision after extensive PRP
- Failure of a tear to seal completely, or development of new tears (after retinopexy)
- Need for additional laser if the disease remains active or recurs
Serious complications are uncommon. The purpose of treatment is to reduce the risk of much more severe outcomes — vitreous haemorrhage, retinal traction, neovascular glaucoma, or retinal detachment.