Flashes and Floaters — When to Seek Urgent Assessment
New flashes of light or a sudden increase in floaters should always be assessed urgently — same day or next day — until a retinal tear or detachment has been excluded.
Most patients who present with these symptoms have a posterior vitreous detachment — a natural age-related change that does not require treatment. But a small number have a retinal tear, and without prompt laser treatment that tear can progress to a retinal detachment requiring major surgery.
The difference between those two outcomes often comes down to how quickly the patient is assessed.
A/Prof Adrian Hunt provides same-day or next-day assessment for new flashes and floaters at Eye Surgeons Miranda in Miranda, or patients can present to Sydney Eye Hospital emergency after hours.

New Flashes and Floaters — See Us Today or Tomorrow
If you have developed new flashes or floaters, or a sudden increase in existing floaters, call the rooms now on (02) 8544 0719. We will see you same day or next day.
Do not wait to see if symptoms settle. A retinal tear can progress to detachment within days, and early treatment is a simple laser procedure. Late presentation may require major surgery.
What Flashes and Floaters Actually Are
The eye is filled with a clear gel called the vitreous. In younger eyes this gel is firmly attached to the retina. With age — often from the mid-40s onwards — the gel begins to shrink and liquefy, and eventually the outer layer peels away from the surface of the retina.
Think of the vitreous as a jelly filling the eye. As we age, the outer skin of that jelly peels away from the retina. Most of the time it comes away cleanly, and that is an uncomplicated posterior vitreous detachment. But occasionally, as it peels, it catches on the retina and pulls a tear. The tear itself can be sealed quickly with laser. If it is not treated, fluid gets through that tear, under the retina leading to a retinal detachment — which is a far more serious problem requiring major surgery.
Floaters are shadows cast on the retina by clumps of vitreous gel or debris that form as the gel collapses. They appear as spots, threads, cobwebs, or rings that move as the eye moves.
Flashes are caused by the vitreous pulling on the retina as it detaches. The mechanical stimulation of the retina is interpreted by the brain as light — commonly seen as brief arcs or streaks in the peripheral vision, often more noticeable in the dark.
Uncomplicated Posterior Vitreous Detachment
The majority of patients who present with new flashes and floaters have a posterior vitreous detachment with no retinal tear — a normal age-related process that does not require treatment.
A PVD without a tear can be identified from the history. Patients often describe a few floaters — often a ring or cluster — and brief arc-like flashes in the peripheral vision, particularly the outer temporal field, that come and go quickly. The flashes are usually short and sharp, like a lightning bolt glimpsed at the edge of vision.
Once a PVD without a tear has been confirmed on examination with pupil dilation, patients can be reassured. The floaters often become less noticeable over months as the brain adapts, though they do not always disappear entirely.
However — and this is critical — the examination must happen first. Symptoms alone cannot reliably distinguish an uncomplicated PVD from one associated with a retinal tear. That distinction requires examination of the retina with the pupil dilated.
About A/Prof Adrian Hunt →When Are Flashes and Floaters a Medical Emergency?
Some symptoms are more worrying than others. Call us same day if you notice any of the following:
- A sudden shower of many new floaters — particularly dark inky streaks
- Flashes that are persistent rather than brief, occasional and reducing in frequency
- A shadow, curtain, or dark area anywhere in your vision — this is an emergency
- Any reduction in vision
- You are significantly short-sighted (myopic) or have previously had cataract surgery
If you have a shadow or curtain in your vision, do not wait — call immediately on (02) 8544 0719.
Why Early Assessment Matters
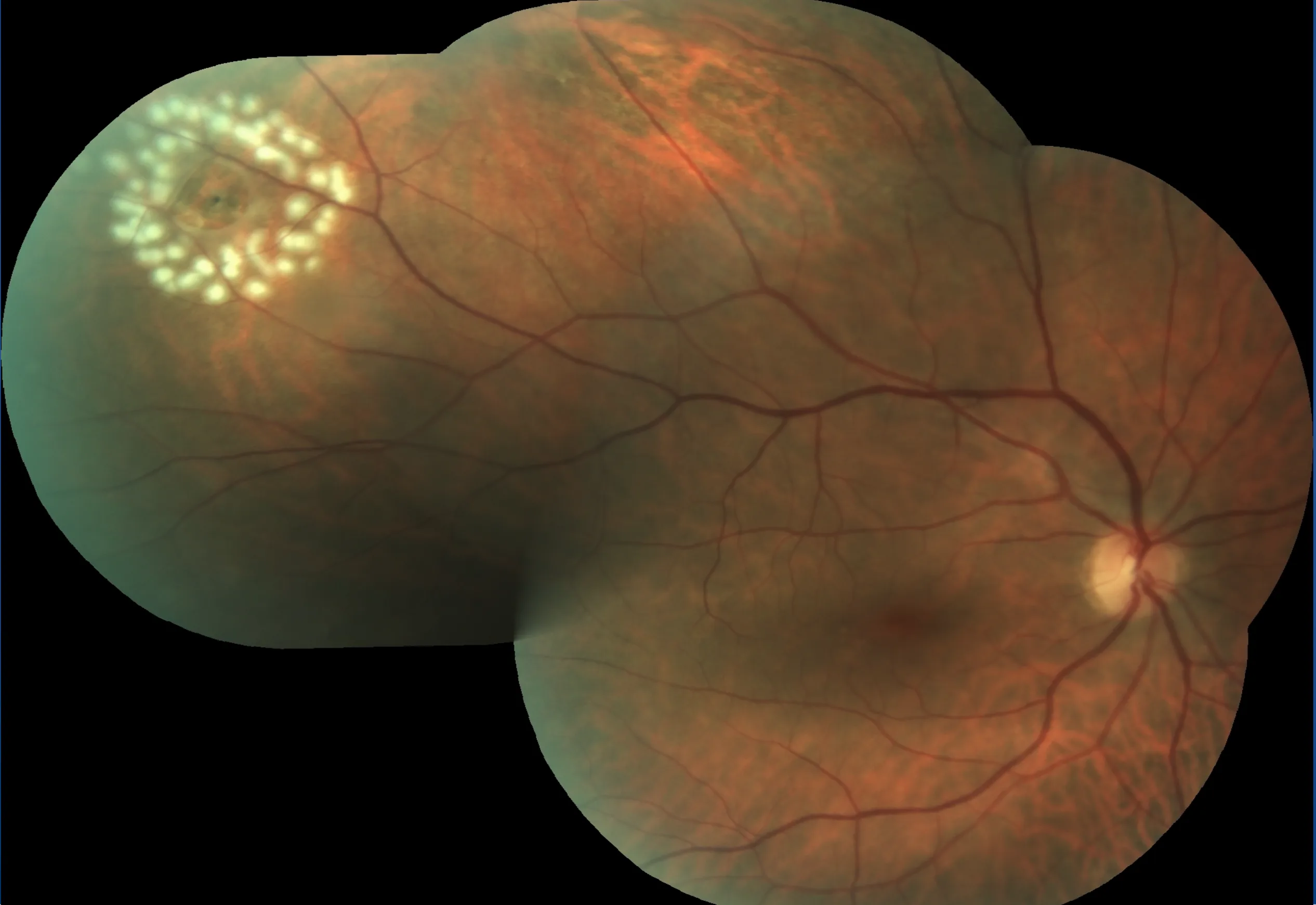
When a retinal tear is found on examination, it can usually be treated immediately with laser retinopexy — a brief, painless in-room procedure that seals the retina around the tear and prevents fluid from passing through.
The laser creates a fence or barrier around the tear, forming a scar that bonds the retina to the underlying tissue. Once healed, this seal is permanent. The procedure is brief and requires no surgery.
What Happens If a Retinal Tear Is Not Treated?
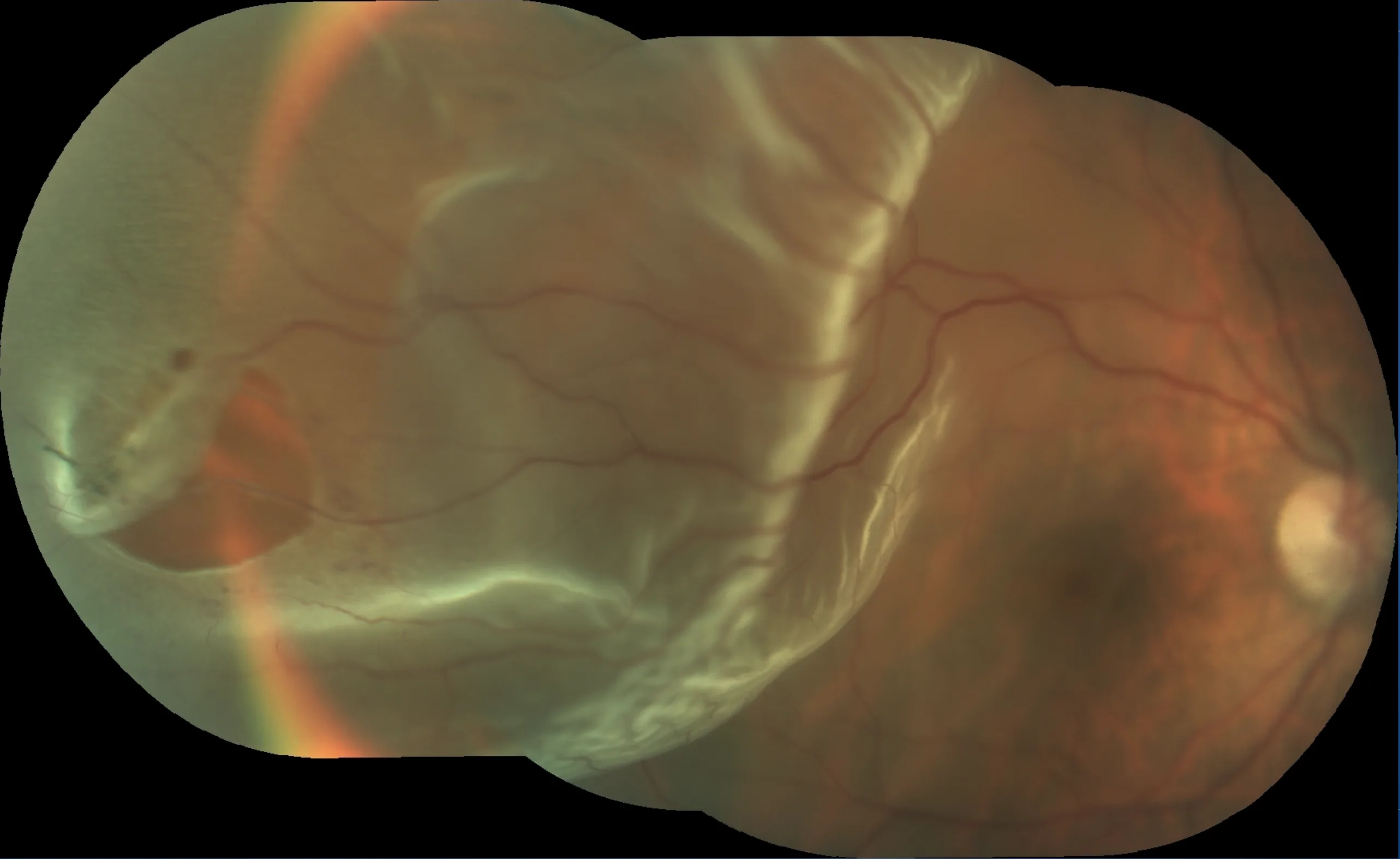
If a retinal tear is left untreated, fluid from inside the eye can pass through the tear and detach the retina — a retinal detachment. A detachment cannot be treated with laser and requires major surgery under general anaesthetic, with a longer recovery and a less predictable outcome.
Chronic Floaters — When They Don't Go Away
For most patients, floaters from a posterior vitreous detachment become less noticeable over weeks to months as they settle further from the retina and the brain adapts. Some patients continue to find floaters bothersome — particularly large, dense floaters that persistently drift across the line of sight.
If floaters remain a significant problem after the acute period has passed, this can be discussed at a follow-up appointment with A/Prof Hunt.
Frequently Asked Questions — Flashes and Floaters
I've had floaters for years — do I still need to be seen?
Long-standing stable floaters that have not changed are much less likely to represent a new problem. However, if you notice a sudden increase in floaters, new flashes, or any change from your baseline, that change should be assessed promptly regardless of your history.
My floaters seem to be settling — should I still come in?
Yes. The floaters themselves settling does not mean a retinal tear is absent — tears do not heal on their own. If you have new flashes and floaters, the retina needs to be examined with pupil dilation to confirm that no tear is present, regardless of whether symptoms seem to be improving.
I only have floaters — no flashes. Is that less urgent?
Floaters without flashes are still worth assessing promptly, particularly if they appeared suddenly or in large numbers. A dense shower of new floaters can indicate bleeding from a retinal vessel at the site of a tear, even without noticeable flashes.
Will I need my pupils dilated?
Yes. A dilated retinal examination is essential to properly assess the peripheral retina for tears. You will need someone to drive you home after the appointment, as dilation affects near vision and light sensitivity for several hours.