Diabetic Eye Disease — Retinopathy, Macular Oedema, and Protecting Your Vision
Diabetes is a blood vessel disease. It can affect every blood vessel in the body, and the retina — with its dense network of tiny vessels supplying one of the most metabolically active tissues in the body — is particularly vulnerable. Over time, those vessels can begin to leak, drop out, or trigger the growth of abnormal new vessels that cause further damage.
The process is gradual, and closely linked to how long you have had diabetes and how well it has been controlled over that time. But one of the most important things to understand is that serious damage can develop silently — vision can be completely normal until suddenly it is not. Regular monitoring is the only way to catch this before it threatens sight.
Almost all the severe vision loss I see from diabetes could have been prevented — by attending regular review.
How Does Diabetes Damage the Eyes?
The two main complications that threaten vision are leakage and loss of blood supply to the retina — and they can occur together.
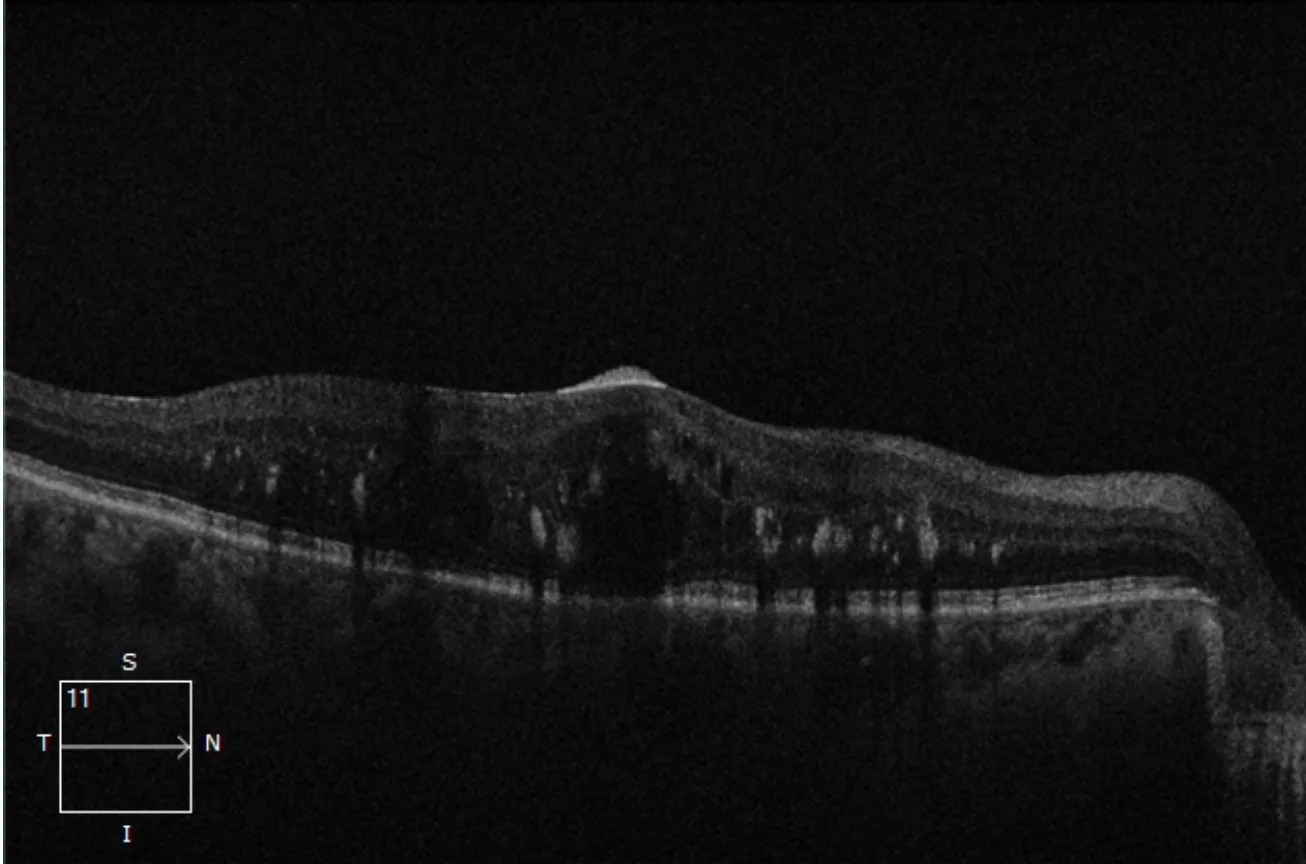
- Diabetic macular oedema (DMO) — damaged vessels leak fluid into the macula, the central part of the retina responsible for detailed vision. The resulting swelling blurs central vision and, if untreated, can cause permanent damage.
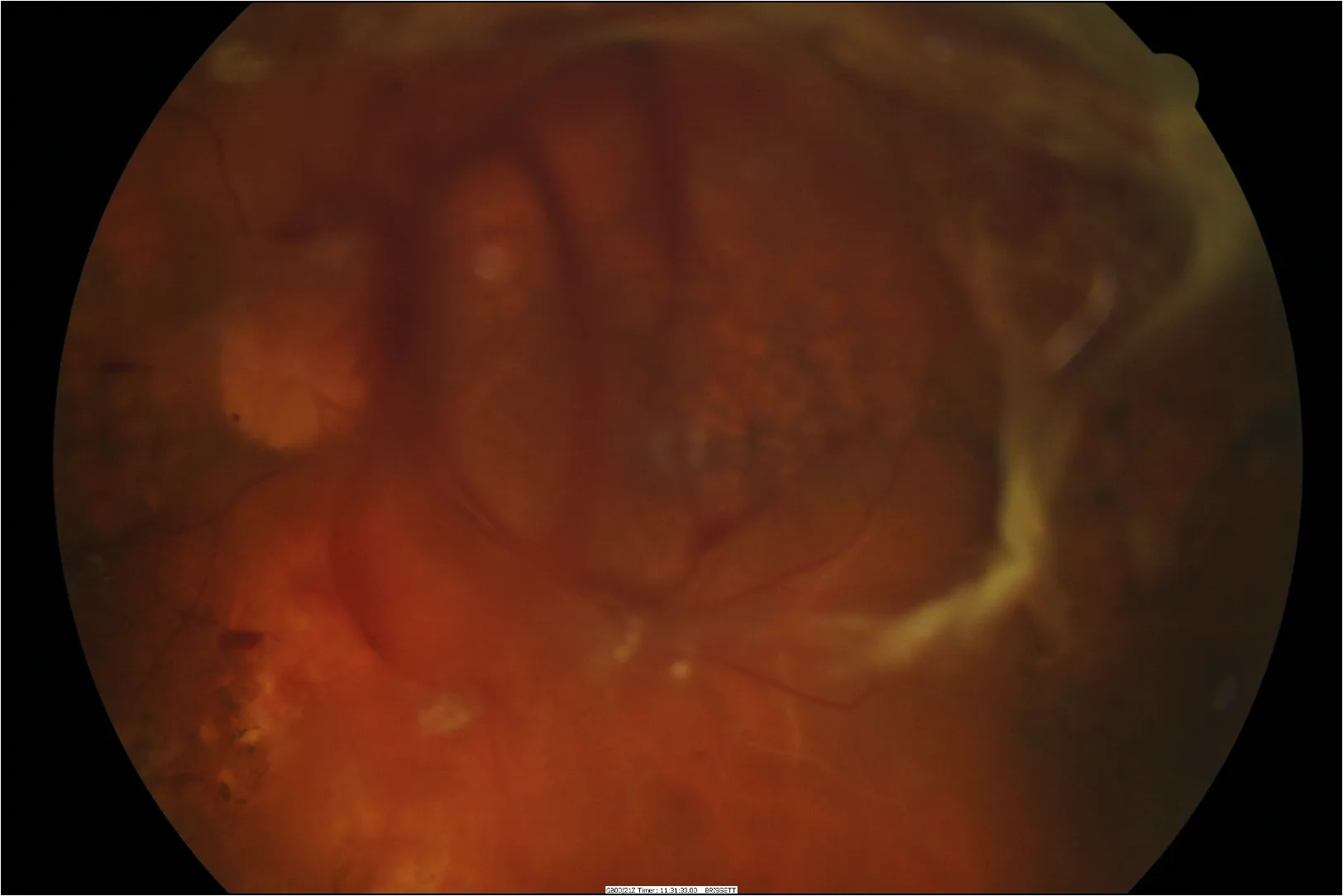
- Proliferative diabetic retinopathy (PDR) — areas of retina that have lost their blood supply become starved of oxygen. In response, the eye tries to grow new vessels to compensate. These new vessels are fragile and prone to bleeding into the eye, causing sudden severe vision loss. They can also pull on the retina and cause a tractional retinal detachment.
Both can develop without warning, but both are treatable — particularly when detected early.
Why Diabetic Eye Disease Often Has No Warning Signs
Proliferative diabetic retinopathy — the more advanced and immediately dangerous form — can develop with no symptoms at all. The abnormal new vessels produce no warning signs until they bleed. When that bleeding happens, the vision loss can be sudden and severe.
This is why waiting for symptoms before seeking eye review is not a safe strategy if you have diabetes. The retina needs to be examined directly — symptoms alone are not a reliable guide to what is happening inside the eye.
Seek Urgent Assessment If You Notice
- A sudden shower of new floaters
- Sudden blurring or loss of vision in one eye
- A dark shadow or veil across part of your vision
These symptoms in a patient with diabetes may indicate a vitreous haemorrhage or retinal detachment and require urgent assessment. Call (02) 8544 0719, or present to Sydney Eye Hospital emergency if after hours.
Stages of Diabetic Retinopathy
Diabetic retinopathy is graded by severity, which guides treatment and how often your retina needs to be reviewed.
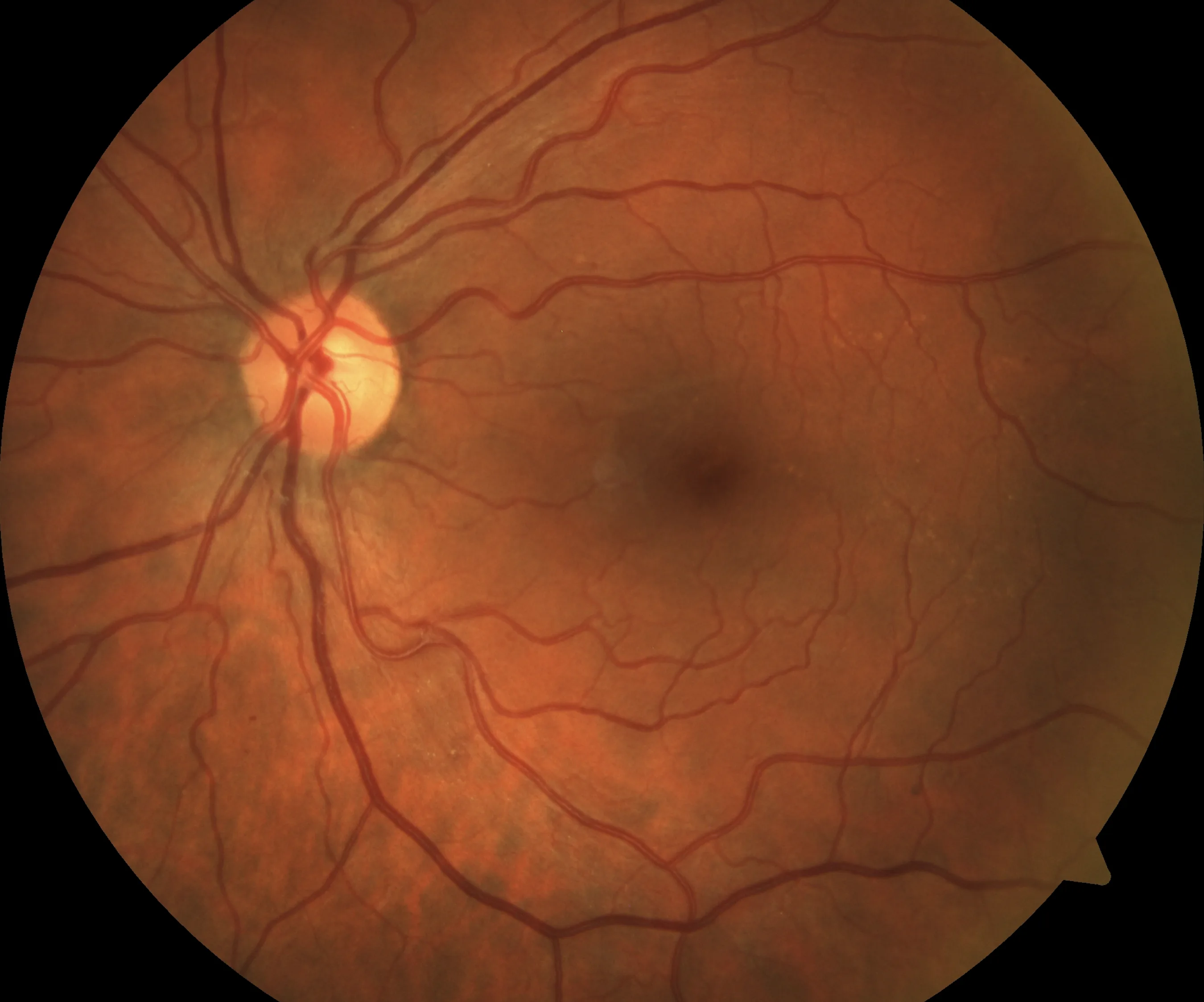
- No diabetic retinopathy — retinal vessels appear normal; ongoing screening is still required
- Mild non-proliferative — early changes such as microaneurysms only
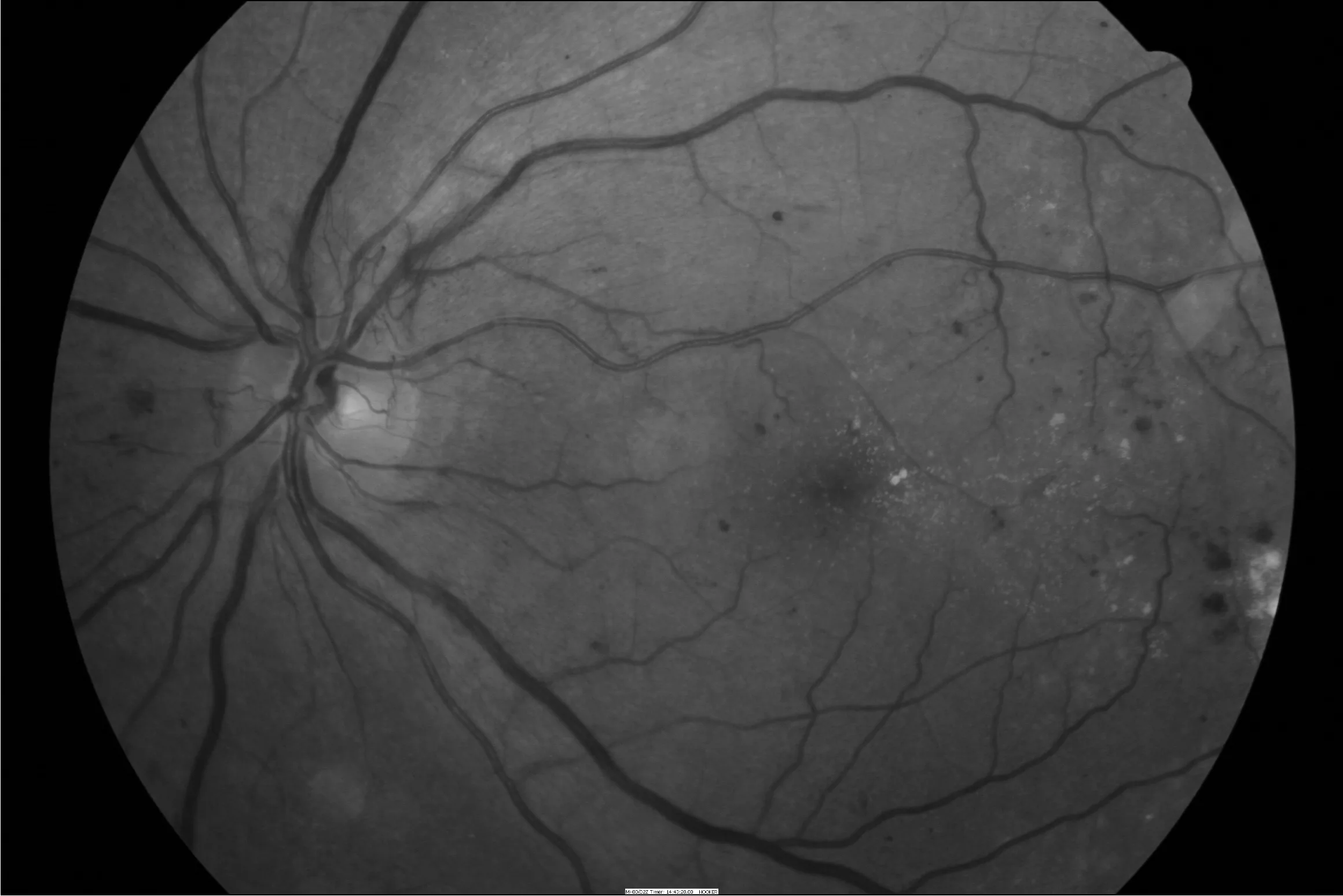
- Moderate non-proliferative — more widespread haemorrhages and exudation, with increasing risk of progression
- Severe non-proliferative — high-risk pre-proliferative disease with a substantial risk of progressing to the proliferative stage
- Proliferative diabetic retinopathy — abnormal new vessels on the retina or optic disc, with risk of bleeding and retinal detachment
- Diabetic macular oedema — can occur at any stage and is assessed separately from the retinopathy grade
Factors that increase the risk of progression include longer duration of diabetes, poor glycaemic control, high blood pressure, renal disease, and pregnancy.
When Should You Have a Diabetic Eye Check?
Every person with diabetes should have a diabetic eye check — sometimes called diabetic eye screening or retinopathy screening — ideally at or around the time of diagnosis, to establish the starting point of their retinal health. How often you need follow-up depends on what is found at that initial review.
More urgent review is appropriate if you have proliferative changes, centre-involving macular oedema, pre-existing retinopathy in pregnancy, or any sudden change in vision.
Diabetic retinopathy is also a marker of wider blood vessel disease. If retinopathy is found, it is worth discussing with your GP or endocrinologist whether your blood glucose, blood pressure, lipids, and kidney function are all being monitored closely.
Treatment — Injections for Diabetic Macular Oedema
Intravitreal injections are the primary treatment for diabetic macular oedema affecting central vision. Anti-VEGF medications reduce vascular leakage, decrease retinal swelling, and protect the macula. In selected cases — particularly where the response to anti-VEGF therapy is incomplete — a steroid implant may be used instead or in addition.
Treatment response is monitored with OCT imaging at every visit, and the schedule is adjusted accordingly.
Treatment — Laser for Proliferative Diabetic Retinopathy
When areas of the retina are starved of oxygen and driving the growth of abnormal new vessels, retinal laser treatment is used to reduce that stimulus. By treating the oxygen-deprived peripheral retina, laser reduces the signal for new vessel growth and protects the eye from bleeding and further complications.
In practice, injections and laser are often used together — injections can rapidly suppress new vessel activity while a course of laser treatment is being completed, reducing the risk of a vitreous haemorrhage during that period.
Learn more about retinal laser treatment →Research in Diabetic Eye Disease
A/Prof Hunt's involvement with the Fight Retinal Blindness! registry includes research on treatment outcomes in diabetic macular oedema — examining how patients respond over years of therapy, when treatment intervals can be safely extended, and what predicts the best long-term vision. This work directly informs the way diabetic eye disease is managed in the consulting room.
See A/Prof Hunt's publications →Diabetic Eye Disease Assessment and Treatment
Eye Surgeons Miranda offers baseline assessments for newly diagnosed patients, ongoing retinopathy monitoring, intravitreal injections for diabetic macular oedema, and laser treatment for proliferative disease. Referrals are welcome from GPs, endocrinologists, and optometrists, and urgent cases are seen promptly.